Suction Machine (Pump) (E 1)
This equipment is mainly important for airway problems as in
Resuscitation of the Young Infant
Subsection of this chapter:
- Clinical Problem
- Assessment
- Management
- Infection Prevention
- Complications
- Care & Maintenance
- Troubleshooting & Repair
NEST360°. Newborn Essential Solutions and Technologies-Education – Clinical Modules: Suction
Pump. (June 2020). License: CC BY-NC-SA 4.0.
Clinical Problem
Obstruction of the nostrils, mouth or upper airway with secretions or blood will cause
respiratory compromise and potential hypoxia.
Suction pumps can be used in patients to clear secretions, vomitus, and blood from the
mouth, nostrils, or upper airway.
LABOUR & OBSTETRIC NOTE
If meconium stained liquor is present at delivery and the baby is not vigorous or has not
taken a breath, inspect the nose and mouth for obstruction. If meconium is present, gentle
suctioning is recommended1. Routine suctioning is not recommended.
Assessment
Suction Pumps
A suction pump (2.1) uses a negative vacuum created by an internal pump to remove
blood or secretions from oral and nasopharyngeal cavities.
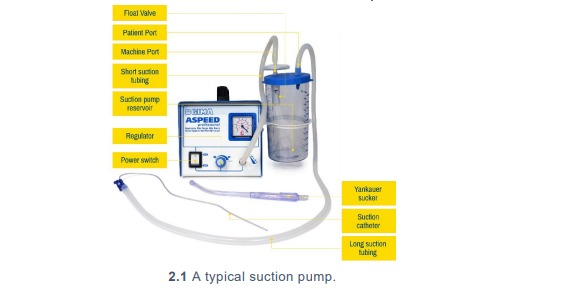
A bacterial filter is used in circuit with the suction pump to filter out any aerosolised particles
or bacteria from the blood and secretions suctioned from a patient.
A suction pump may be tailored to adults (2.2) or paediatric (2.3) patients.

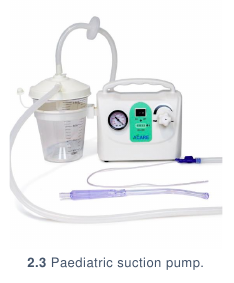
Although an adult suction pump can be used on paediatric or neonatal patients, the vacuum range is much
higher which makes it more difficult to control for the low ranges required for neonatal
patients. Use of an adult pump to treat neonatal patients is not encouraged.
Penguin suckers
Penguin suckers are reusable devices made of a flexible silicone, which can be used to
provide low pressure suctioning.(2.4) Penguin suckers are autoclavable. Although suction
bulbs may also be used, they are not autoclavable, sare difficult to clean, and are not
recommended due to greater infection risk between patients.


Neonatal patients should be suctioned gently, no deeper than the eye can see and only
within a range of 60 to 100 mmHg of negative pressure and for a period less than 10
seconds. (Alert 2.1)
| ? |
ALERT 2.1 Suction Efficacy |
In the referenced document, WHO recommends a range of 50-100 mmHg
for suctioning for no more than 10 seconds. Based on expert feedback, it
was felt that 60-100 mmHg is likely a more effective range and still within
the WHO recommendation.2 |
Management
Management covers how to use the suction pump, including set up for a patient,
patient preparation & commencement, care whilst on the device & removal of the
patient from the device.
SETTING UP FOR A PATIENT
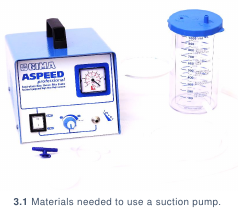
- Collect: (3.1)
- Suction pump with collection reservoir
- Suction pump filter (if not already attached to pump)
- Short suction tubing
- Long suction tubing
- Suction catheter or Yankauer sucker
- Water in a suitable container (e.g., kidney dish, bowl)

- Visually inspect the suction pump’s collection reservoir. If it is full or there are secretions
present (3.2), dispose of the secretions appropriately, clean the reservoir and place it back
in place with the lid firmly closed.
- If a filter is not attached to the collection reservoir, place the filter in the lid of the collection
reservoir at the port labelled
Vacuum
. Using the short suction tubing, connect the inlet
of the suction filter on the suction pump collection reservoir to the suction pump outlet port.
(3.3)
- Connect long suction tubing to the collection reservoir outlet port labelled
Patient.
(3.4)
- Plug the power cable in the device. (3.5) Plug the power cable into the wall and turn on
suction pump.



- Connect the suction catheter or Yankauer sucker to the long suction tubing. (3.6)
- Using the suction regulator, adjust the suction vacuum to the desired level within safe
neonatal levels (60 to 100 mm Hg). Test the suction functionality with
some water. (3.7)
PREPARING A PATIENT
- Collect: (3.1)
- Suction pump with collection reservoir
- Suction pump filter (if not already attached to pump)
- Short suction tubing
- Long suction tubing
- Suction catheter or Yankauer sucker
- Water in a suitable container (e.g., kidney dish, bowl)
- Always explain the purpose, risks, and benefits of a procedure to guardians BEFORE
performing the procedure. Follow handwashing protocol and put on gloves.
- Suctioning is only required when there is airway obstruction. Visually inspect the patient’s
oral and nasopharyngeal cavities for secretions or blood.
- Assess whether to use a suction catheter or Yankauer sucker.
- For thicker secretions it may be necessary to use a Yankauer sucker but do not
use in the nares of a newborn.
- For thinner secretions, use an appropriately sized suction catheter (typically Fr
sizes 6, 8 or 10). A correctly sized suction catheter should be the approximate size
of the nostril. Nasogastric tubes are not recommended as a substitute for a suction
catheter.
- If secretions, blood, or meconium are visible, collect:
- Clean suction catheter or Yankauer sucker
- Tape
- If using a suction catheter: determine suction depth by measuring from the nose to the ear
and halfway back. Mark this distance with a small piece of tape. (3.8)
- If using a Yankauer sucker, no measurement is required. Suctioning should only be
conducted as far as can be visually assessed.
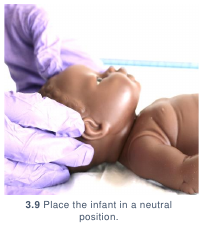
- Place the infant in a neutral position to ensure effective suctioning. (3.9)

STARTING A PATIENT
- Collect: (3.1)
- Suction catheter marked with appropriate suction depth or Yankauer sucker
- Suction pump with collection reservoir and tubing in place
- Water in a container
- Always explain the purpose, risks, and benefits of a procedure to guardians BEFORE
performing the procedure.
- Follow handwashing protocol.
- Plug suction machine into power outlet and turn on.
- Connect suction catheter marked with appropriate suction depth or Yankauer sucker to
long suction tubing. (3.11)
- Using the suction regulator, adjust the suction vacuum to the desired level, maintaining
safe vacuum levels for neonates. Test the suction functionality by suctioning the water.
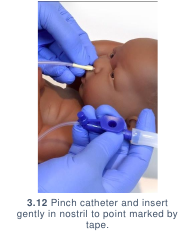
- When using a suction catheter: pinch the catheter and insert gently into the patient’s
mouth or nostril to the point marked by the tape. When introducing catheter into the nose
do so following the floor of the nose. Release the pinch on the catheter slowly as you
withdraw the catheter from the mouth or nostril, gently rotating until it is completely
removed. (3.12)
- If using a Yankauer sucker: for thicker secretions or meconium, it may be necessary
to use a Yankauer sucker.
- Suctioning should only be conducted as far as can be visually assessed when
using a Yankauer sucker. If secretions are thick, application of 1-2 drops of normal
saline to both nostrils may assist suctioning and reduce nasal trauma.
- Some Yankauer suckers may require a hole at the hub of the sucker to be occluded
for suctioning pressure.
- Allow the patient to visibly recover from the procedure. While waiting, rinse the catheter
with water. Repeat this process on the other side of the mouth or nostril.
- Repeat steps 5 through 7 until all secretions are removed. Remember: suctioning
should be a gentle procedure. Do not suction too vigorously and do not suction too
long. Suction only until the reservoir is ¾ full; if it reaches this point, remove collection jar,
dispose of contents and reattach to complete suctioning.

CARING FOR A PATIENT
Observe suctioned contents carefully whilst suctioning procedure is taking place:
- If fresh blood starts to be suctioned, trauma may have been caused to the oral or
nasopharyngeal cavities. Decrease the force with which the suction catheter is being
inserted into the patient’s nose or mouth.
- If stomach contents are being suctioned, the patient’s suction catheter is being inserted
into the oesophagus. Recheck the suction depth measurement.
REMOVING A PATIENT
Gently withdraw the suction catheter from the patient’s passageway.
Infection Prevention
Routine and adequate cleaning of medical devices is critical to prevent hospital�acquired infections in newborn care units. If devices & equipment are not
disinfected promptly & adequately between patients, they pose a significant
infection risk.
GENERAL INFECTION PREVENTION
- Clean hands with soap and water or alcohol before and after initiating treatment
using a suction pump or handling any tubing that will be used on a patient.
- Ensure that all patient-related tubing and consumables (including suction catheters
and collection reservoirs) are new or have been cleaned thoroughly before use (if
following re-use guidelines). Any patient-related tubing must be cleaned (following
the ward protocol) before it is used to suction another patient. Tubing should be
hung to dry after disinfection and should not touch the floor or other unsanitary
surfaces whilst drying.
- When re-using suction tubing there is a risk of infection if inadequately cleaned. If
the machine is not cleaned after each use, it can become a source of infection for
patients in the ward. Suction catheters should never be reused.
- All patient-related consumables should be stored in a clean, dry location. Tubing
should be stored in loose rolls, preventing sharp bends and kinks, which will
decrease its lifetime.
| ! |
ALERT 4.1 |
Electrical suction pumps and associated equipment, if not re -processed
or cleaned appropriately between patients, pose a significant infection
risk. Please refer to WHO Technical Specifications for Resuscitation
Equipment chapter 2.6 or Infection Prevention and Control: Reference
Manual for Health Care Facilities with Limited Resources, Jhpiego
Module 6 for more detailed guidance on reprocessing of equipment
associated with suction pumps.2,3 |
DISINFECTION AFTER USE
- Gently disconnect the suction catheter from the suction tubing and dispose of
catheter appropriately. If reusing, immediately begin hospital protocol for
disinfection of tubing. Delay in initiating cleaning of reused medical devices
can lead to the need for more intensive cleaning procedures to remove
pathogens. If not reusing, discard safely.
- Turn off and unplug the suction pump, if not using with another patient. Check filter.
If filter is obviously dirty, replace. (4.1) Refer to user manual for specific instructions
on when to change the filter.
- Disinfect the suction pump pressure gauge controls using gauze and 70% alcohol.
- The housing of the suction pump should be cleaned according to ward guidelines
for disinfecting surfaces.
- All tubing and collection reservoir should be cleaned after each patient.
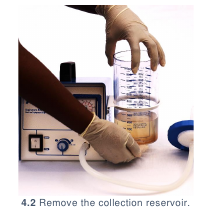
- Remove the collection reservoir from suction pump. (4.2) Dispose of contents and
disinfect reservoir appropriately, wearing gloves, a mask and apron to ensure staff
safety. Return collection reservoir to suction pump and store in secure location until
next use.
- Remove short and long suction tubing pieces. Follow hospital protocol for disinfection
of tubing.

Complications
Introduction of equipment in newborn care units poses clinical and device
complications for patients. Awareness of potential complications is critical to
maximise patient safety.
CLINICAL COMPLICATIONS
- Hypoxia: if a patient is on oxygen, it may be necessary to remove oxygen treatment during
suctioning, especially when suctioning the oropharynx. This interruption in treatment may worsen
patient’s hypoxia. Place the patient back on oxygen as soon as oral and nasopharyngeal cavities
are clear.
- Trauma: incorrect or excessive suctioning of the nose and mouth may cause trauma to mucosal
surfaces. (This is more likely to happen when the pressures on the machine is above the safety
range for neonates 60-100mmHg.) If bleeding occurs, stop suctioning, assess severity, and
restart when safe.
- Vomiting: incorrect measurement of the suction catheter or suctioning too far may stimulate the
gag reflex and induce vomiting. This also risks potential aspiration.
- Vagal stimulation: inappropriately deep suctioning can cause vagal stimulation resulting in
apnoea or bradycardia.
DEVICE COMPLICATIONS
Positioning:suction pumps are not heavy devices but are frequently positioned on walls /
shelves. This is appropriate if well secured during use. If improperly secured, suction pumps may
fall, causing potential permanent or fatal injury, particularly to neonatal patients.
Care & Maintenance
Users are responsible for basic first-line care and maintenance to ensure
equipment lasts to their potential lifetime.
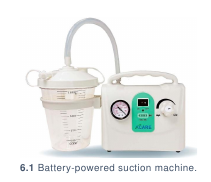
POWER SOURCE
Suction pumps may be powered by mains or battery power (6.1) or manually via a foot or
hand pump. (6.2) If a suction pump is battery powered, it should be taken off its charger
only as necessary to ensure that it is charged for use in the event of a power blackout.

WARD LOCATION
Suction pumps should be secured in an accessible location where nursing staff can
regulate and view vacuum easily, but where the pump is not at risk of falling. Suction
consumables should be kept nearby for easy access in case of emergency.
USER PREVENTIVE MAINTENANCE
The suction pump should be turned on and allowed to run for 15 minutes every week.
Troubleshooting & Repair
Although users are not responsible for repairing their devices, there are steps that
may be taken to troubleshoot first-line errors that may occur before contacting
maintenance or engineering support.
| 1 |
The device does not turn on |
|
- Check that the machine’s power cable is firmly secured (7.1)
and that the power at the socket is on. If it is loose, secure the power cable.
- If the machine still does not turn on, contact your maintenance team.
|
| 2 |
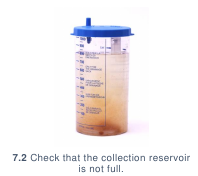
The device stops suctioning |
|
- Suction pumps often have a fail-safe valve installed in the lid of the
collection
reservoir to ensure that fluid is not sucked into the machine’s internal pump.
Check that the collection reservoir is not full (7.2); if it is, empty
and continue
procedure.
- Check that the tubing is not loose and leaking. If the machine still does not
suction, contact your maintenance team. |

References
- Helping babies breathe provider guide. (American Academy of Pediatrics, 2016).
- WHO technical specifications for neonatal resuscitation devices. (World Health
Organization, 2016).
- Curless MS, Ruparelia CS, Thompson E, and Trexler PA, eds. 2018. Infection Prevention
and Control: Reference Manual for Health Care Facilities with Limited Resources.
Jhpiego: Baltimore, MD.