
After completion of this chapter the participant should be able to:
HIE is also called birth asphyxia and neonatal encephalopathy, and in this document, we will use the term HIE. HIE is very common in Malawi; therefore, the optimal management of these newborns is very important.
Lack of oxygen supply to organs before, during, or immediately after birth, results in HIE which is recognized by either delayed onset of breathing or crying. Clinical features that evolve in these babies over the first 2-3 days of life include irritability, lethargy or coma, hypotonia or hypertonia of the muscles, convulsions, apnoea, temperature instability, poor suck, and feeding difficulty. The diagnosis in preterm infants is difficult, as they may be hypotonic because of prematurity.
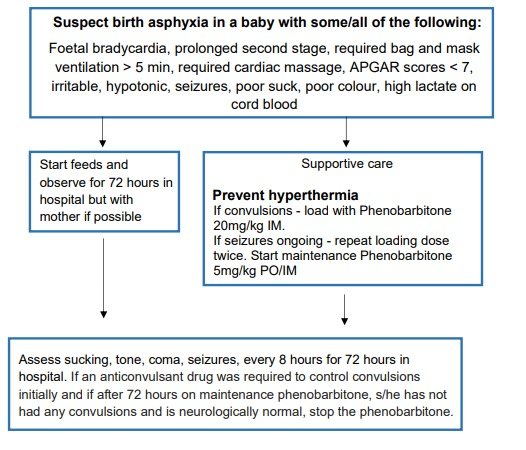
Suspect HIE in a baby with some/all of the following:
Classify the degree of Hypoxic Ischaemic Encephalopathy (HIE) according to the table below. Babies with mild and moderate HIE generally have a good prognosis and do well. A newborn who, within a week of birth, is still floppy or spastic, unresponsive, and cannot suck has severe brain injury and will do poorly.
| Feature | Mild | Moderate | Severe |
| Consciousness | Irritability | Lethargy | Comatose |
| Tone | Hypotonia | Marked hypotonia | Severe hypotonia |
| Seizures | No | Yes | Prolonged |
| Sucking/ respiration |
Poor suck | Unable to suck | Unable to sustain adequate regular spontaneous respiration |
Distinguishing Between Convulsions and Jitteriness
Most children with HIE present with convulsion; however, these are often subtle and need to be differentiated from jitteriness. The table below shows how convulsions can be differentiated from jitteriness.
| Convulsions | Jitteriness |
| Have both fast and slow components; slow movements (1-3 jerks per second). | Fast movements (4-6 per second); tremors are of equal amplitude. |
| Not provoked by stimulation. | Provoked by stimulation. |
| Does not stop with restraint. | Stops with restraint. |
| Neurological examination often abnormal. | Neurological examination usually normal. |
| Often associated with eye movements (tonic deviation of the pupil) or blinking. | Not associated with eye movements or autonomic changes. |
| Key Facts for Providers: Supportive Management of Birth Asphyxia |
|---|
|
Documentation, Discharge and Follow-up
Document in health passport and classify HIE as mild, moderate, or severe.
If severe, arrange for a physiotherapy appointment (initially floppy infants often become stiff requiring the mother to learn massage and basic physiotherapy skills) and follow up at six months - focus on head growth, general health, and motor neurodevelopment. Assessments at 12 to 24 months focus on cognitive skills and language development.